Worker Discomfort Survey
For printable version users can fill out, download this resource.
Completed by:
Date:
Job name:
Shift:
Department:
Time on job:
Please list other jobs you have done in the last year (for more than two weeks).
Note: If more than two jobs, only include those you worked on the most
Questions:
- Have you had pain or discomfort during the last year that you feel is job-related? (Yes/No)
If no, stop here. If yes, please rate the level of discomfort over the last month by checking off the appropriate box using the scale of 0 to 10, with 0 being no discomfort and 10 being the worst discomfort ever.
Image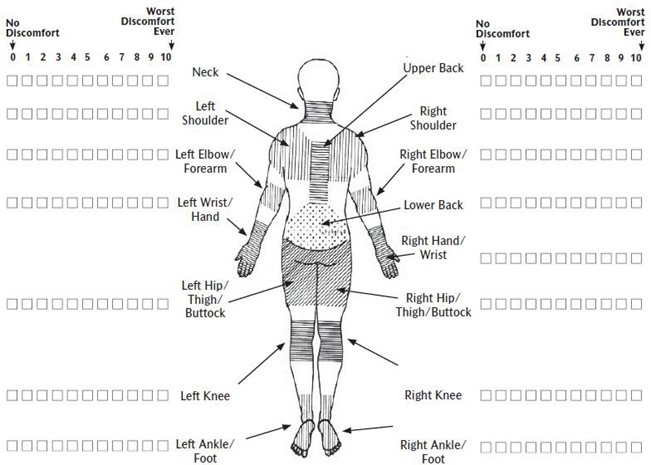
- When did you first notice your discomfort? (indicate month, year)
- What do you think caused the discomfort?
- Please comment on what you think would help to reduce your level of discomfort.
- Do you consider your discomfort to be a problem? (Yes/No)
- Have you received medical treatment (from a doctor, chiropractor, physiotherapist, massage therapist or other health care practitioner) for your discomfort? (Yes/No)
- Have you taken time off work because of your discomfort (vacation, sick days, lost time claim, medical aid)? (Yes/No)
Content sourced from the MSD Prevention Guideline for Ontario, Part 3B: MSD Prevention Toolbox (2007)